During labor at a Florida hospital, a pregnant mother of three was brought before a judge via Zoom court for refusing a C-section. Despite her concerns about previous difficult recoveries and the low statistical risk of uterine rupture, medical professionals believed a C-section was necessary for the safety of her and her baby. The court ultimately ruled that the hospital could perform a C-section in an emergency without her consent, and she later underwent the surgery. This case highlights the contentious issue of forced medical treatment for pregnant individuals and the potential conflict between a mother’s autonomy and the perceived welfare of the fetus.
Read the original article here
It’s truly a stark and disturbing scenario when a woman in the throes of labor finds herself on a Zoom call in court, her fundamental medical decisions being debated and ultimately overridden. This situation, unfolding in Florida, highlights a deeply unsettling intersection of healthcare, law, and individual autonomy, raising profound questions about patient rights and the extent to which the state can intervene in deeply personal medical choices, particularly during childbirth.
The narrative paints a picture of a woman, who had arrived at the hospital with a clear birth plan, seeking a vaginal delivery. However, her background as a professional birthing doula, a role that inherently involves navigating the complexities and unpredictability of labor, also meant she understood that plans can change. This understanding, however, did not prepare her for the legal entanglement that awaited her.
The core of the issue seems to stem from the hospital’s push for a C-section, a procedure the woman was understandably hesitant to undergo, especially given her history. Yet, when she expressed her refusal, instead of facilitating a dialogue or ensuring robust advocacy, the situation escalated to a court hearing. The fact that Florida law, in this specific context, did not mandate or provide an attorney or advocate for the pregnant woman concerning her medical decisions is a critical point of concern. This left her in a vulnerable position, facing a panel of medical professionals and legal minds, while lying in a hospital bed, connected to monitors, and with limited ability to articulate her reasoning.
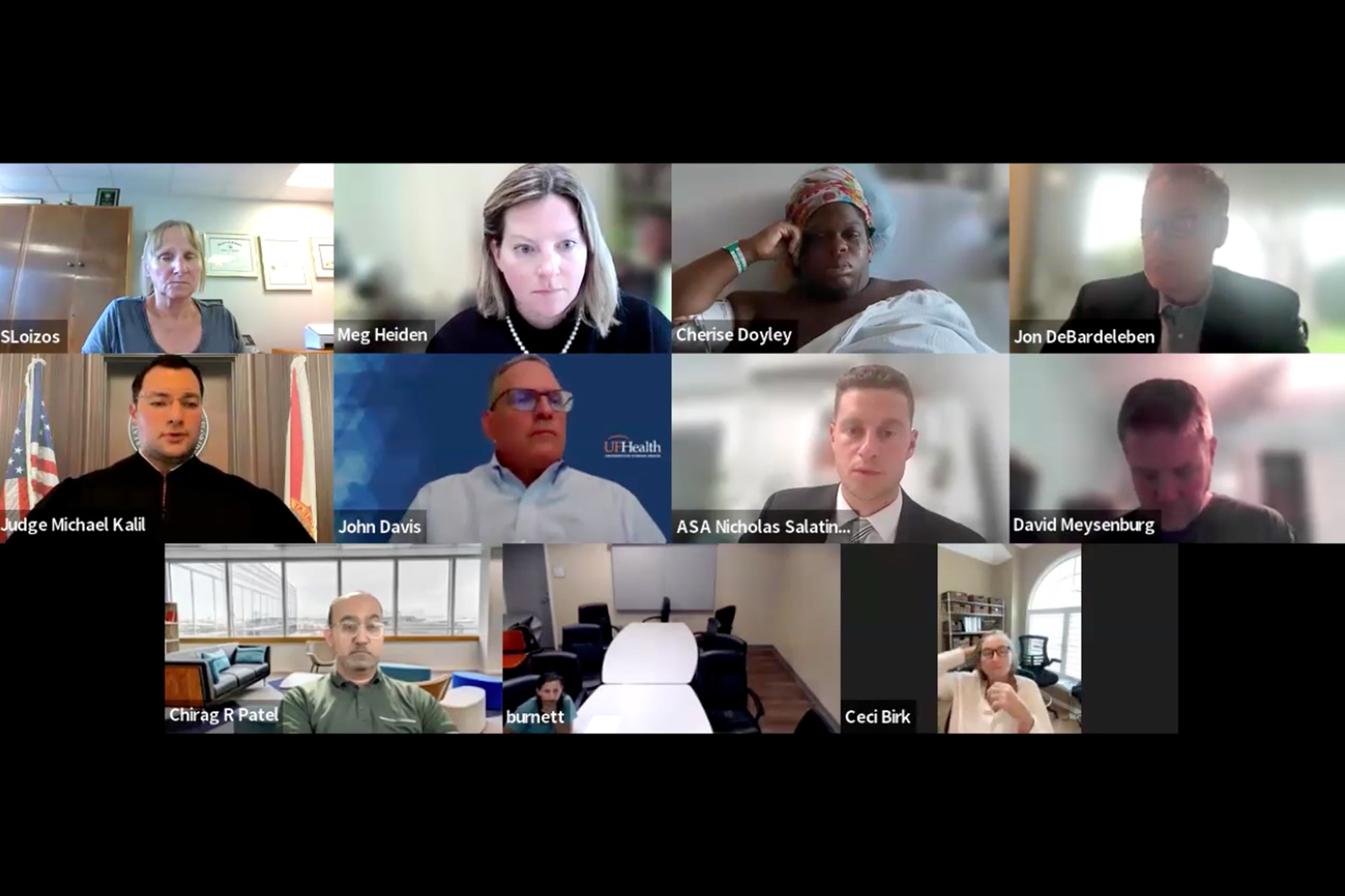
The imagery of her on screen, surrounded by numerous doctors and lawyers, most of them appearing to be white, while she, a Black woman, was hooked up to IVs and monitors, is particularly striking. The focus of the testimony, as presented, centered heavily on the potential risks to the baby if the C-section wasn’t performed, while seemingly giving less weight to the documented downsides the mother faced from previous C-sections, such as recovery challenges, infection risks, and even the possibility of death. The inability to immediately voice her concerns, being on mute for a significant portion of the hearing, only adds to the feeling of disempowerment.
This case brings to the forefront the concept of informed consent, a cornerstone of medical ethics. When a patient’s refusal of a medical procedure leads to a court order and the potential for a forced intervention, the very essence of “informed consent” is severely challenged. The swiftness with which the court convened and a judge made a ruling over a woman’s bodily autonomy, while she was actively in labor, feels deeply invasive and indicative of a system that, in this instance, prioritized a perceived medical necessity over the patient’s expressed wishes and rights.
The broader societal implications are also significant. The commentary touches upon the idea of women being viewed as mere “incubators” rather than individuals with agency over their own bodies. The fear of moving backward, especially in terms of reproductive rights and bodily autonomy, is palpable. This situation feels like a dystopian narrative, reminiscent of the scenarios depicted in speculative fiction where individual liberties are overridden by state control.
Furthermore, the comparison drawn to other legal situations, where significant delays or inaction occur despite clear evidence of wrongdoing, highlights a perceived imbalance in the legal system’s responsiveness. The urgency with which this woman’s medical decision was brought before a judge, contrasted with the perceived slowness in addressing other serious societal issues, raises questions about priorities and the application of legal resources.
The fact that she was denied a lawyer or an advocate in a hearing that would directly impact her body and her child’s birth is particularly egregious. The argument that a patient in active labor is not in a state to competently participate in a court hearing, especially one where their most intimate medical decisions are being scrutinized, is a valid point of contention. The contrast drawn with situations involving religious objections to life-saving treatments underscores the complex ethical and legal terrain surrounding medical decision-making when parental autonomy clashes with perceived medical best interests.
Ultimately, this case serves as a disturbing example of how a healthcare system, potentially influenced by a confluence of factors including legal frameworks, institutional liability concerns, and deeply ingrained societal biases, can erode individual autonomy at a moment of profound vulnerability. The legal and ethical ramifications of forcing a medical procedure against a patient’s will, especially when that patient is in the midst of labor and has expressed clear reasons for their refusal, are profound and warrant serious consideration and re-evaluation.